Did you know?
Right now, lawmakers can support more than 100 New York hospitals and their patients – at no cost to the state.
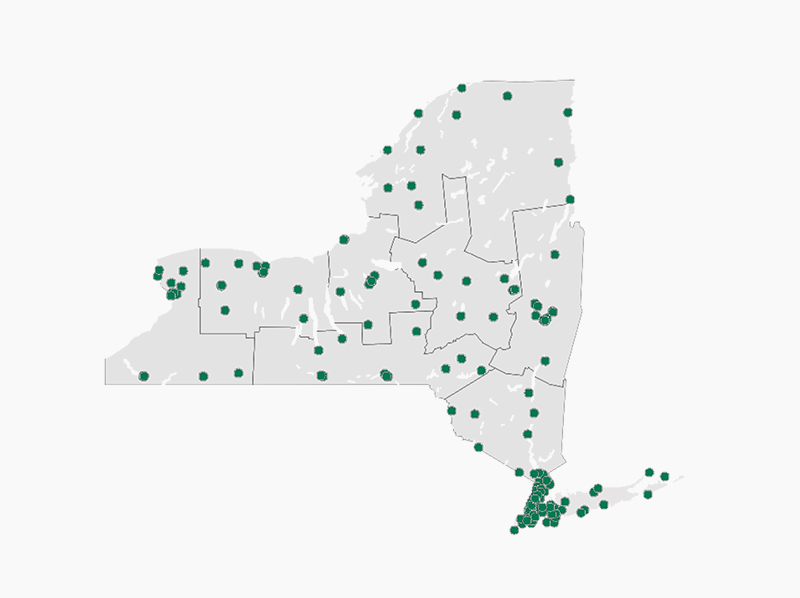
Click on the map to see New York’s 340B hospitals
Show all participating hospitals
The federal 340B Drug Discount Program is a cornerstone of New York’s healthcare safety net. Established in 1992, the program allows eligible hospitals, health centers and other “covered entities” to purchase outpatient drugs at discounted prices from drug manufacturers. Providers reinvest the savings from these discounted drug purchases to sustain operations and invest in patient care.
340B does exactly what Congress intended: it reduces provider costs as a way of funding healthcare services without using additional federal funding.
Today, that safety net is under threat. For-profit drug manufacturers, pharmacy benefit managers and others are creating barriers that intentionally undermine providers’ ability to fully benefit from 340B savings. They are restricting the use of contract pharmacies and imposing burdensome and discriminatory practices that weaken safety net providers and jeopardize New Yorkers’ access to care.
The 340B Prescription Drug Anti-Discrimination Act would stop these harmful actions.
It would prevent drug manufacturers from blocking safety net providers’ use of contract pharmacies. It would also prohibit them from adding unfair fees, penalties and administrative hurdles that undermine the 340B program.
The bill would not expand the 340B program. It would simply stop enormously wealthy pharmaceutical companies from chipping away at it and hold them to their commitment to support the cost of providing care to New York’s most vulnerable patients.
340B has no direct impact on patient costs. Hospitals do not set drug prices – drug manufacturers do. Nothing in the federal 340B statute prohibits multi-billion-dollar drug manufacturers from issuing more discounts or making drugs cheaper for New Yorkers.
340B also has no impact on hospital reimbursement for drugs. These reimbursements are set by government and commercial payers and PBMs.
The 340B Prescription Drug Anti-Discrimination Act would not regulate prices. It would protect critically needed resources intended to enhance patient access to care.
Protecting 340B also protects the state budget. 340B drug discounts are funded entirely by drug manufacturers and represent only a small share of pharmaceutical industry revenue. When these savings are eroded, hospitals and other providers are forced to turn to the state government to help make up the shortfall.
New York would not be acting alone. States across the country have already acted to stop for-profit drug manufacturers and others from circumventing 340B requirements to increase their profits at the expense of patient care.
Amid chronic and new challenges facing our healthcare providers and patients, we are grateful to New York’s lawmakers who have advanced many budget and legislative proposals aimed at strengthening the state’s healthcare system. Protecting 340B is one of those proposals – and it must advance.
The bottom line: Protecting 340B is one of the best tools available to protect New Yorkers’ access to care.
We urge New York lawmakers to include the 340B Prescription Drug Anti-Discrimination Act in the FY 2027 enacted budget.
Learn more about 340B:
-
What is the 340B program?
Established in 1992, the 340B Drug Pricing Program allows certain eligible healthcare organizations, known as “covered entities,” to purchase outpatient drugs at discounted prices from drug manufacturers. 340B covered entities reinvest their savings to improve patient access to care in underserved communities.
-
What is the 340B program’s intent?
This essential program helps eligible healthcare providers enhance access to care in their communities.
Per House Report No. 102-384(II) that accompanied the 340B Drug Pricing Program legislation in 1992 (P.L. 102- 585), “In giving these ‘covered entities’ access to price reductions the Committee intends to enable these entities to stretch scarce Federal resources as far as possible, reaching more eligible patients and providing more comprehensive services.”
Per the federal district court opinion in “AbbVie Inc. v. Drummond” (2025), “Congress enacted the 340B Program … to help qualifying healthcare providers (“covered entities”) stay afloat by allowing them to purchase certain outpatient drugs from manufacturers who participate in Medicaid and Medicare Part B at a discount negotiated by the Secretary of Health and Human Services.”
-
Who participates and benefits from 340B?
Covered entities include:
- disproportionate share hospitals;
- children’s hospitals;
- cancer hospitals;
- Critical Access Hospitals;
- Sole Community Hospitals;
- Rural Referral Centers;
- FQHCs;
- Ryan White HIV/AIDS clinics;
- state AIDS Drug Assistance Programs; and
- other federally-supported safety net providers.
More than 100 hospitals across New York state and the patients they serve benefit from 340B, as these healthcare providers reinvest their savings into new and enhanced healthcare programs and services for their patients.
More than 150 drug manufacturers participate in 340B. Drug manufacturers benefit because, in return for participating in 340B, their products are eligible for reimbursement under Medicare and Medicaid, a large share of the U.S. prescription drug market.
-
How do 340B hospitals use their savings?
Eligible hospitals leverage savings accessed under 340B to operate programs and services that they might otherwise not be able to offer, such as:
- free or substantially discounted prescriptions to uninsured or low-income patients;
- medication therapy management programs to improve patient care and reduce overall healthcare costs and hospital readmissions;
- mobile units to bring care to rural and other medically underserved communities without local primary care options or pharmacies;
- free oncology services for low-income patients;
- HIV/AIDS clinics; diabetes management programs;
- multidisciplinary clinics offering substance use disorder and mental health services; and
- transportation support for patients who need emergency room and chronic care services.
-
What are contract pharmacies?
Contract pharmacies are off-site retail or specialty pharmacies partnering with 340B hospitals to dispense drugs to patients. Contract relationships are the only way for hospitals to dispense drugs at off-site pharmacy locations.
-
What harmful actions are impacting 340B providers and their patients?
Drug manufacturers, pharmacy benefit managers and others are unilaterally working to limit hospitals’ ability to optimize 340B through restrictive/discriminatory requirements.
For example, they are placing limits on 340B participation by restricting how far a contract pharmacy can be from a covered entity and capping the number of allowable pharmacy partners, sometime to one or even none. They are also imposing extra burdens on 340B hospitals, such as:
- added fees;
- clawbacks;
- dispensing charges;
- network restrictions;
- inventory system mandates; and
- excessive data submission requirements.
These reduce 340B savings for hospitals providing care to vulnerable communities. Instead, savings intended for safety net providers are being shifted to massive for-profit entities. This is creating a distressing funding gap for 340B providers that state and/or federal governments may need to fill.
-
What would S.1913 (Rivera) / A.6222 (Paulin) do?
The 340B Prescription Drug Anti-Discrimination Act would prevent the blocking of 340B contract pharmacy arrangements. It would also prohibit special rules or payment terms for 340B hospitals that differ from other hospitals and/or pharmacies.
-
Have other states acted to protect 340B?
Yes! More than 20 states have acted to protect contract pharmacy arrangements; nearly 30 have acted to protect 340B providers from discriminatory practices by drug manufacturers and PBMs.
Additional resources: